The admin load behind a busy practice
A small practice carries a load that a hospital network spreads across whole departments. With ten to two hundred staff, the same handful of people answer the phone, manage the diary, process claims, chase recalls and keep the records straight, often while patients wait. Allied health and dental clinics feel it just as sharply, with one reception desk holding the whole operation together.
The pressures are specific. Reception runs the phone, the inbox and the waiting room at once. Clinicians finish consultations and then write up notes into the evening. No-shows and last-minute cancellations leave paid time empty. Recalls slip, claims sit unsubmitted, and intake forms get filled in by hand during the appointment that should be spent on care. None of this is clinical work, yet it eats the hours that clinical work needs.
Underneath all of it sits a duty no other sector matches. The data is among the most private a person has, and the practice answers to AHPRA, to the Privacy Act and to its own clinical governance. So the question is never how to go faster. It is how to ease the load without ever putting a patient or their information at risk.
Why a single app rarely fixes it
The instinct is to buy a booking app or a note tool, switch it on, and hope. A fortnight later reception is logging into one more system, the note tool drafts something nobody trusts, and patient data has quietly travelled somewhere no one signed off on. The tool was never the problem. How it was set up was.
Three things separate software that quietly earns its keep from software that becomes a liability, and none of them come in the box.
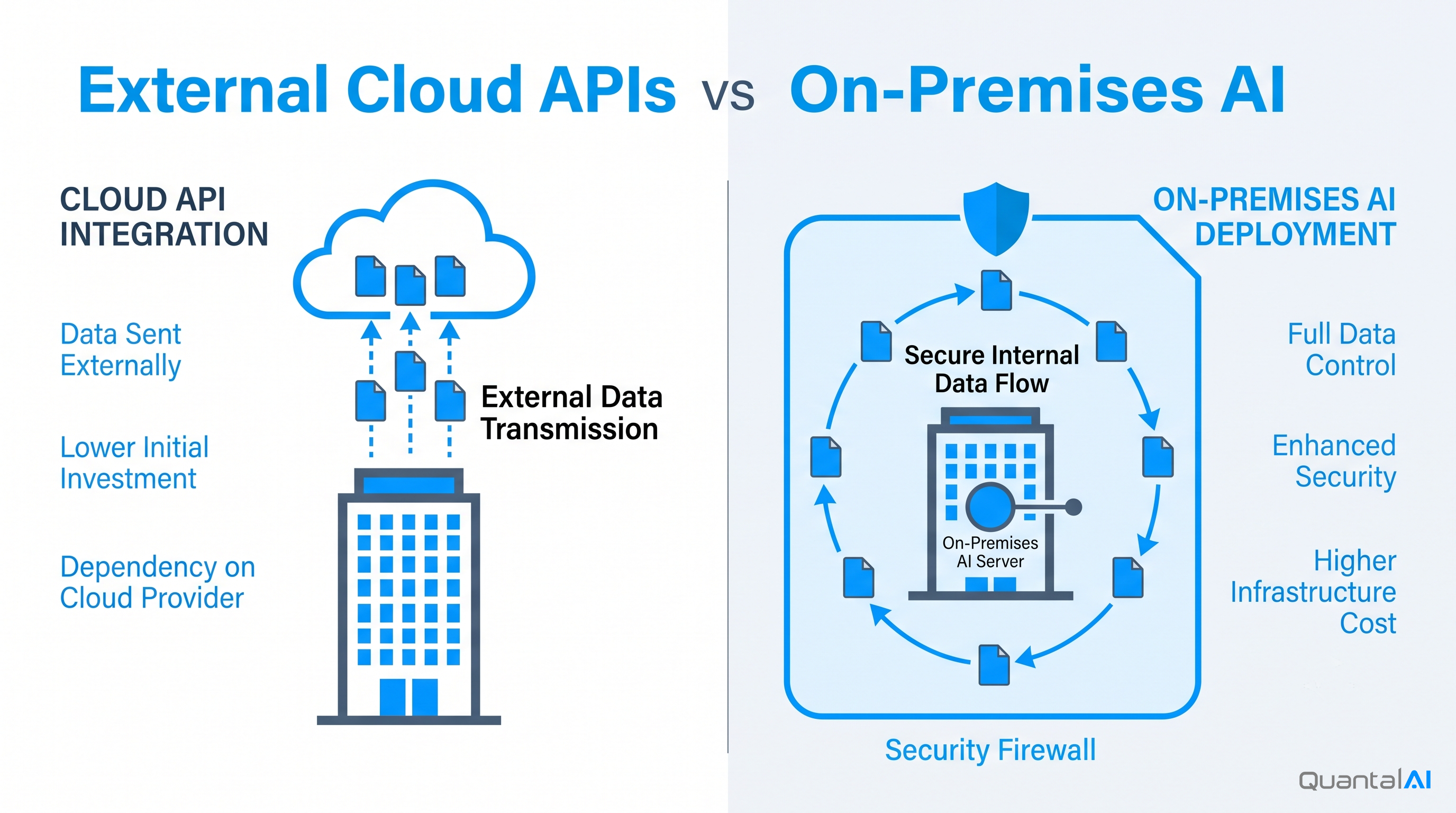
It has to put patient privacy and governance first. A tool near patient care cannot be a black box. We lead with training, security and governance, so each tool only sees the data it genuinely needs, patient information stays where it should, and nothing leaves for a third-party service without your explicit agreement. We design around the Privacy Act 1988 and the Australian Privacy Principles, respect the access and consent rules attached to My Health Record, and build so your practice can stand behind it to AHPRA and to a patient.
Anything touching care has to be auditable. When a tool drafts a note or surfaces a referral, you need to show what it did and why. We keep the prompts, the data each tool can reach and the design choices behind it under version control, the same way we manage code. Every change is recorded, and if a change makes things worse we roll it back. That documented, versioned process is what satisfies clinical governance, rather than a tool nobody can explain.
It has to give time back, not add clicks. A tool that makes reception fill in three more fields has failed. We start from the job that costs your team the most time, usually note drafting or the front desk, and build around how your people already work. If a simpler automation does the job better than AI, we will tell you and build that instead.
These are the foundations we insist on. You can read more about them in our approach.

How we put it to work
We work in small, reviewable steps rather than one big switch-on, so risk stays low and you see value early. We pick one job where the load is heaviest and a mistake is recoverable, agree what good looks like, and connect the tool to the practice management and clinical software you already run through secure interfaces. We keep a clinician or a staff member in the loop, with the tool drafting or proposing and a person reviewing, until you trust it. Prompts, access and decisions go under version control from the start. Then we test against your own real cases, measure where it helps, release to a small group and expand once it holds.
For most practices the first job is note drafting or the front desk. The note tool prepares a summary or referral letter from the consultation for the clinician to edit and sign, so documentation stops running into the evening. The front-desk tools handle bookings, reminders, recalls and the waitlist, so reception spends less time on the phone and fewer paid slots sit empty. Intake moves to before the visit, billing and claiming get chased automatically, and a patient’s history becomes searchable. Through all of it the clinical decision stays with the clinician, and a human reviews anything that reaches a patient.
What changes for your practice
The outcome we aim for is hours returned to care and a calmer front desk. Documentation that ran into the evening is drafted in moments for review and sign-off. Reminders and an actively managed waitlist cut no-shows and fill cancellations, so paid time is not lost. Recalls and claims stop slipping. Patients arrive with intake already done, and staff find the record they need without scrolling through years of history.
In every case the practice keeps full control of patient data and of every clinical decision, with a logged trail to show how a tool was used. We are deliberately careful here. A tool you cannot trust around a patient is no tool at all, and a named clinical reviewer signs off before anything goes live. We build for safety and privacy first, and for speed within those bounds.
A practice, not a hospital
Smaller practices often feel the load most sharply, because there are fewer people to absorb it. We build for that reality rather than scaling down a hospital platform. We start with the burden that costs your clinicians and reception the most time, build something focused around it, and keep your clinicians in control of care while the admin gets lighter.